GENERAL MEDICINE
25/09/2023 13 year female with fever
September 24, 2023
Hi, I am Pindi Gayatri, 5th sem medical student. This is an online E-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
CONSENT AND DE-IDENTIFICATION :
The patient and the attenders have been adequately informed about this documentation and privacy of the patient is being entirely conserved. No identifiers shall be revealed throughout this piece of work whatsoever.
Chief Complaint:
13 year female resident of Nalgonda student by occupation came to opd with chief complaints of
-Fever since 5 days
History of Present Illness:
-Patient was apparently asymptomatic 5 days ago then she developed fever which is high grade associated with chills and rigors.
-No diurnal variation and no aggravating and relieving factors accompanied with Headache ,generalized myalgia, sore throat ,loss of appetite.
-c/o dark coloured stools
-no c/o cough,cold,SOB
-no c/o burning micturation
-no c/o loose stools, nausea and vomiting
Daily Routine:
Before she got sick, she used to wake up at 6 am every morning, take a bath at 6.30am, eat breakfast of rice and curry and leave for school by 8.30am. She used to reach home by 5 or 6 pm after which she would study for sometime, eat and sleep by 11pm.
After she got sick, she stopped going to school and stayed at home, following which she was admitted into the hospital.
Past History:
No similar complaints in the past
Not a k/c/o DM, HTN, Thyroid
Surgical history:
-H/o Tonsillectomy 8 years ago
Personal History:
- married: single
- appetite lost
- mixed diet
- bowels : constipation
- normal micturition
- no known allergies
- addictions: no known addictions
Family History: not significant
Drug History:
-Dolo 500 mg
General Examination:
I have examined the patient after taken prior consent and informing the patient in the presence of a female attendant. The examination was done in both supine and sitting position in a well lit room.
- patient was conscious, coherent and cooperative
- well oriented to time and space
- well built and adequately nourished
- no pallor
- no icterus
- no cyanosis
- no clubbing of fingers
- no lymphadenopathy
- no edema of feet
- no malnutrition
- no dehydration
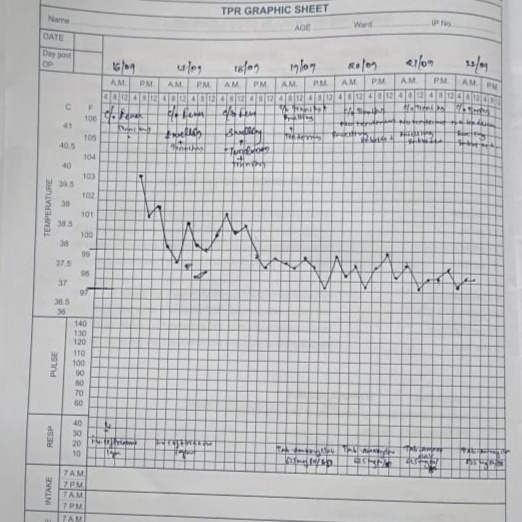
Vitals:
- Temperature: afebrile
- Pulse: 60 beats/min
- RR: 16 cycles/min
- BP: 100/70 mm Hg
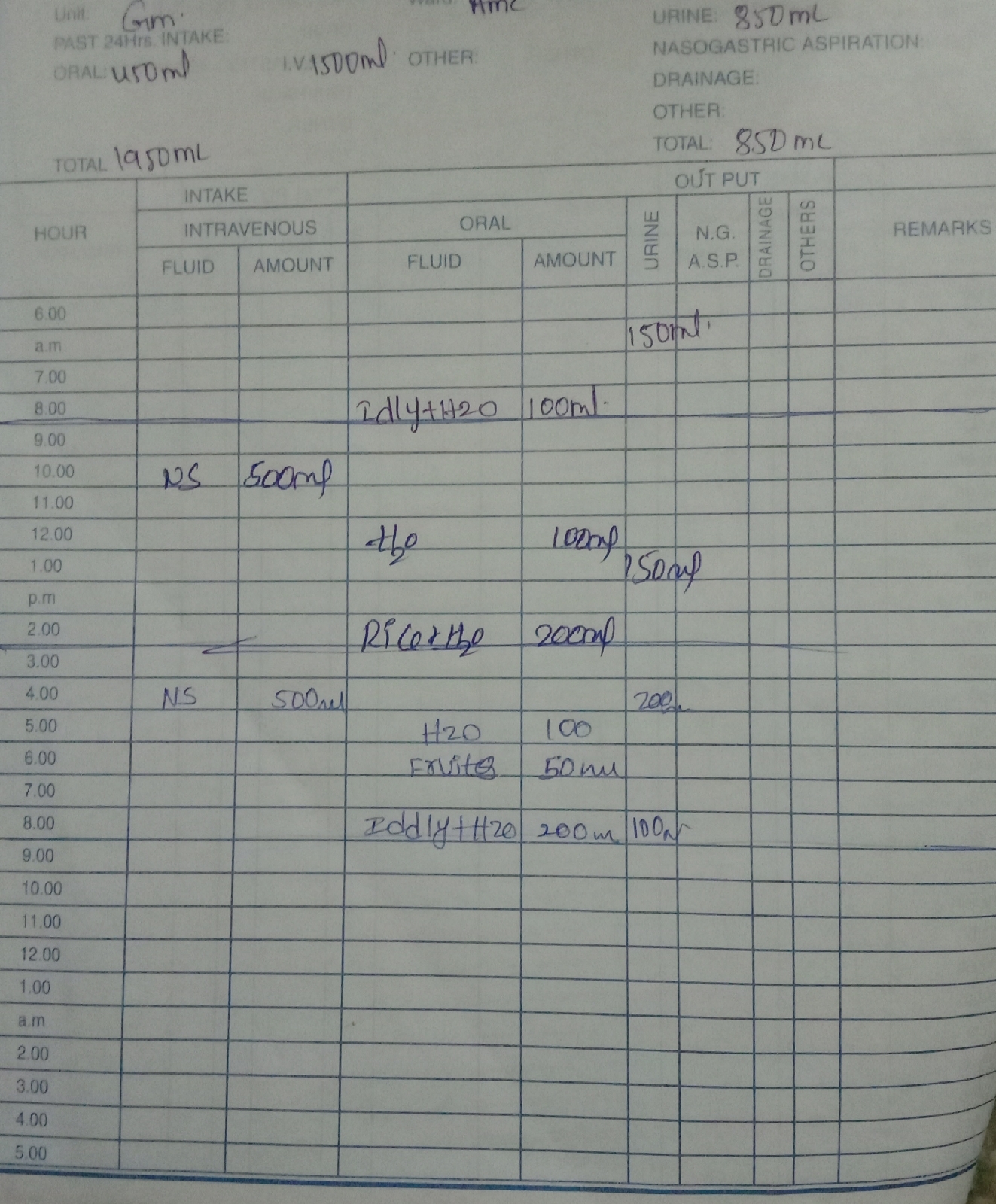
Fluid Intake and Urine Output
Systemic Examination:
Respiratory System
- upper respiratory tract : nose & oropharynx appear normal,oral cavity petechiea present
- chest is bilaterally symmetrical
- respiratory movements appear equal on both sides and of thoracoabdominal type
- position of trachea : central
- vesicular breath sounds : present
- no wheeze
Cardiovascular System:
Inspection :
- shape of chest : elliptical
- no engorged veins, scars, visible pulsations
Palpation :
-Apex beat can be palpable in 5th intercostal space
- no cardiac thrills
Auscultation :
- S1,S2 are heard
- no murmurs
Abdomen:
- shape: scaphoid
- no tenderness
- no palpable mass
- no bruits
- no free fluid
- hernias orifices: normal
- liver: not palpable
- spleen : not palpable
- bowel sounds: yes
- genitals:normal
- speculum examination : normal
- P/R examination : normal
Central Nervous System:
- conscious
- normal speech
- no neck stiffness
- no Kerning's sign
- cranial nerves: normal
- sensory : normal
- motor: normal
- reflexes: all present bilaterally
BICEPS TRICEPS SUPINATOR
RIGHT +2 + +
LEFT +2 + +
KNEE ANKLE
RIGHT. +2 +2
LEFT + +
- finger nose in coordination: not seen
- knee heel in coordination: not seen
- gait: normal
Investigations:
22/09/2023
-Hb: 11.2
-PCV: 35.5
-TLC: 3000
- WBC: 4.06
-Platelet count: 2.82
-B.urea: 15
-S.creatinine: 0.7
-S.Na+: 136
-S.k+: 3.7
-S.cl: 99
-SGPT: 11
-SGOT: 26
-Alk.phosphate: 341
-T.protein: 6.7
-Albumin: 3.98
-A/G ratio: 1.46
23/09/2023
-PLT: 1.71 L
24/09/2023
-Hb: 11.6
-PCV:35.5
-TLC:3400
-PLT:1.5 L
25/09/2023
-Hb:12.1
-PCV:37.6
-TLC:5400
-PLT: 1.55 L
ECG:

Provisional Diagnosis:
-Dengue NS 1 Positive
Treatment:
1.IV FLUIDS NS-75 ML/HR
2.INJ.NEOMOL 500 MG IV/SOS
3.INJ.MONOCEF 500 MG IV/BD
4.INJ.FALCIGO 120 MG IV
5.TAB.DOXYCYCLINE 100 MG PO/BD
6.TAB.PCM 650 MG PO/TID