GENERAL MEDICINE
58 year female with headache since 2 months
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
CONSENT AND DE-IDENTIFICATION :
The patient and the attenders have been adequately informed about this documentation and privacy of the patient is being entirely conserved. No identifiers shall be revealed throughout this piece of work whatsoever.
Chief complaints:
58 year old female patient resident of Suryapet daily wage laborer by occupation came to OPD with chief complaints of headache since 2 months.
HISTORY OF PRESENT ILLNESS:
H/o trauma to head 2 months ago
Patient was apparently asymptomatic 2 months ago then she had a h/o of taruma with lacerations over parietal region for which suturing was done,from then she had h/o of headache which was throbbing pain, continuous,non-radiating accompanied by burning sensation of eye and lacrimation of eyes.
No h/o blurring of vision
No h/o nausea and vomiting
No h/o seizures, diplopia
Daily Routine:
Before she got sick, she used to wake up at 5am every morning, cook for her and her husband, take a bath at 6.30am, wash clothes and dishes by 8am, eat breakfast of rice and curry and leave for work by 8.30am. She is a daily wage laborer by occupation and she used to pack lunch which was the same rice and curry as breakfast and eat it at her workplace. She used to reach home by 7 or 8pm after which she would cook dinner of rice and curry, eat and sleep by 11pm.
After she got sick, she stopped going to work and stayed at home, following which she was admitted into the hospital.
PAST HISTORY:
Similar complaints of headache in the past - gives h/o fall
C/o left foot pain with pus discharge - h/o thron prick
C/o left sided lower back pain non
radiating since 8 years gives h/o fall.
Not k/c/o DM,TB,Asthma,CAD
Surgical history: Hysterectomy was done 15 years ago
Personal History:
- married
-normal appetite
- mixed diet
- regular bowels
- normal micturition
- no known allergies
- addictions: toddy drinker once in 6 months.
Family History: not significant
Drug History:
TAB.Calcium carbonate and vit D3
TAB.NAXOS-D 500mg
TAB.Cefredrox-CV
General Examination:
I have examined the patient after taken prior consent and informing the patient in the presence of a female attendant. The examination was done in both supine and sitting position in a well lit room.
- patient was conscious, coherent and cooperative
- well oriented to time and space
- well built and adequately nourished
- no pallor
- no icterus
- no cyanosis
- no clubbing of fingers
- no lymphadenopathy
- no edema of feet
- no malnutrition
- mild dehydration
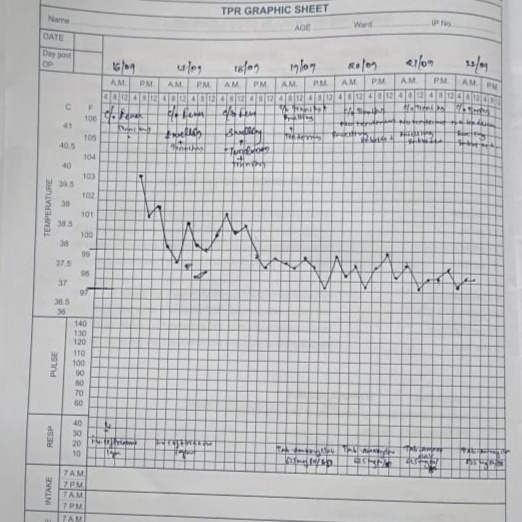
Vitals:
- Temperature: afebrile
- Pulse: 76beats /min
- RR: 20 cycles/min
- BP: 110/70 mm Hg
-SPO2:98%
Systemic Examination:
Respiratory System
- upper respiratory tract : oral cavity, nose & oropharynx appear normal
- chest is bilaterally symmetrical
- respiratory movements appear equal on both sides and of thoracoabdominal type
- position of trachea : central
- vesicular breath sounds : present
-no wheeze
Cardiovascular System:
Inspection :
- shape of chest : elliptical
- no engorged veins, scars, visible pulsations
Palpation :
-Apex beat can be palpable in 5th intercostal space
- no cardiac thrills
Auscultation :
- S1,S2 are heard
- no murmurs
Abdomen:
- shape: obese
- no tenderness
- no palpable mass
- no bruits
- no free fluid
- hernias orifices: normal
- liver: not palpable
- spleen : not palpable
- bowel sounds:yes
- genitals: normal
- speculum examination : normal
- P/R examination : normal
Central Nervous System:
- conscious
- normal speech
- no neck stiffness
- no Kerning's sign
- cranial nerves: normal
- sensory : normal
- motor: normal
- reflexes: all present bilaterally
- finger nose in coordination: not seen
- knee heel in coordination: not seen
- gait: normal
-Skin:Scar on parietal region
INVESTIGATIONS:
Hemogram

Bleeding and clotting time

Urine examination

HIV 1/2Rapid Test

HBsAg-Rapid

Anti-HCV Antibodies -Rapid

USG

ECG

PROVISIONAL DIAGNOSIS:
Chronic headache secondary to post trauma USG of left foot showed 2mm hyperechoic foci noted in left plantar aspect,surgery was done foreign body is removed
TREATMENT:
TAB.Paracetomol 40mg
TAB.HIFENAC-P
TAB.LIMCEE 500mg