General Medicine
A 14 year old boy with multiple clinical events.
27,August, 2022
E LOG GENERAL MEDICINE
Hi, I am Pindi Gayatri, 3rd Sem Medical Student.This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.”
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
CHIEF COMPLAINTS
A 14 year old male came to hospital with the chief complaints of swelling in the left sided abdomen since 15 days.cold,cough since 10 days.
HISTORY OF PRESENT ILLNESS
Patient is 4th order child ,born out of grade 4 consanguinous marriage.He has 2 elder brothers and one elder sister -who expired at 5 years of age.His sister was the first child , she was asymptomatic till 2 years of age,then she had shortness of breath and was rushed to hospital where her condition deteriorated &got admitted.
They were told that she had splenomegaly &her blood counts were decreasing.she was given multiple blood transfusions every 25 days for 1 year,inspite of that she remained anemic,she also underwent bone marrow biopsy twice.According to the parents she was given steroids also for 1 year before death.she never had jaundice or recurrent infections.
Elder brother is 19 year old and second brother is 16 years old. Second one had history of fever,white colored loose stools at the age of 5 years,for which they went to hospital. He was given some medications & it got resolved.But he was said to have anemia,and he recovered according to parents with some medications.There was no jaundice and no history of blood transfusion.
Patient history:
He is the youngest of all.He was born out of normal vaginal delivery with 4 kgs of birth weight,cried immediately after birth.He had jaundice at birth,that resolved spontaneously? physiological jaundice.
He is immunized as per schedule.
At 8 months age : patient had history of altered bowel habits - 1 week of loose stools and 1 week of normal consistency stoolsfor few days later he was passing loose stools everyday for 2-3 months,during which he became very cachetic.He got admitted in the hospital, in the discharge summary-they mentioned as suspected case of ?coeliac disease,?chronic diarrhoea.
During hospital stay he was given IV antibiotic and 2 FFP transfusions.He recovered in 3 months according to parents.
On further asking parents told he used to have recurrent colds,cough and fever.He used inhalers for 1 year during winters in childhood, though he was not admitted at any point ,and there was no history of pneumonia.
At 9 years of age parents noticed neck swelling and took him to ENT doctor later referred to endocrinologist,where he was diagnosed with hypothyroidism (TSH 150),he was started on 150 mcg thyronorm ........later increased to 180 mcg thyronorm.
History of chronic itching over hands and foot since age of 9 years.
At 12 years of age ,he had chicken pox,resolved over 10 days.
At 13 years of age(Jan 2022)he has complaints of yellowish discoloration of eyes for 10 days with 1 episode of bilious vomiting and complaints of yellowish colored urine.
No pale colored stools,no fever,pain abdomen, loose stools,no cold,cough.No history of small joint pains.
O/E: He was thin built .
Jaundice +pallor +per abdomen-moderate splenomegaly.
Outside investigations
There is significant drop in hb from 8.9 to recent hb-5.
Leucopenia,thrombocytopenia with raised bilirubin-both direct and indirect.,normal enzymes.
Urine fir bile salts+bile pigments+ve Hb electrophoresis-normal.
Serology-for HiV,HBSag,HCV was negative.
Dengue,malaria, widal test was negative.moderate splenomegaly.
Since 15 days ,he is noticing swelling in the abdomen for which he was diagnosed to have massive splenomegaly.
He had ulcer over right leg.patient was apparently asymptomatic 4 days ago,then developed a boil which ruptured to form an ulcer.
O/E : ulcer (0.5×0.5 cm)over lateral aspect of right leg.,no discharge.
Sloping edges,local rise of temperature, tenderness, peripheral pulses.
HISTORY OF PAST ILLNESS
It is a known case of hypothyroidism since 6 years
It is not a known case of epilepsy, Asthma, CAD, tuberculosis, etc.
TREATMENT/DRUG HISTORY
No Diabetes mellitus
No hypertension
No Hyperthyroidism
No CAD
No asthma
No tuberculosis
No antibiotics
No hormones
No blood transfusion
No surgeries

PERSONAL HISTORY
Single
Occupation-student
Habits/addictions -Alcohol-teetotaler
FAMILY HISTORY
History of thyroidism of his grandparents(grandmothers from both sides I.e.,mother and father side)
GENERAL EXAMINATION
Patient is coherent,conscious,cooperative,
well oriented to time,place and person.
He is moderately built and moderately nourished.
pallor is seen
No icterus
No cyanosis
No clubbing of fingers/toes
No lymphadenopathy
edema of feet is present
No dehydration.






VITALS
Temperature-98.8 °F
Pulse rate- beats-84/min
Respiratory rate- times-18/min
Blood pressure-100/70 mmHg( left arm)
Spo2-98%at room air at RA litres of O2
SYSTEMIC EXAMINATION
CVS
No thrills
S1S2 Cardiac sounds heard
No cardiac murmurs
RESPIRATORY SYSTEM
Position of trachea-central
Normal vesicular breath sounds heard
No dyspnea
No wheezing
ABDOMEN
Shape-scaphoid
No tenderness
No palpable masses
No hernial orifices
No free fluid
No bruits
No bowel sounds heard
palpable spleen and liver
CNS
Level of consciousness-conscious/alert
Speech- normal
Signs of meningeal irritation
No stiffness of neck
Kerning's sign:negative
Reflexes
Plantars-flexor
Cerebral signs
Finger nose In-coordination:No
Knee heel In-coordination :No
PROVISIONAL DIAGNOSIS
AIHA
INVESTIGATIONS

On 24th, August



On 26th, August




On 27th, August

Ultrasound report



At 6:44am



At 8:38am

 pain abdomen (dragging type).
pain abdomen (dragging type).
On 28th, August
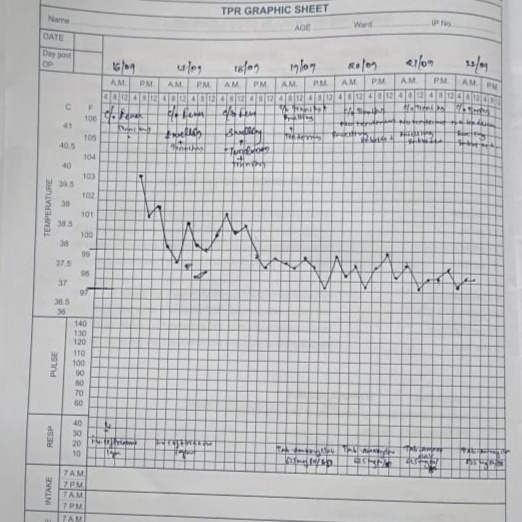
Cough decreased,fever spikes are present,stools passed.
29th, August
Pain abdomen, fever spikes absent stools passed.
30th & 31st, August
Pain abdomen (dragging type),fever spikes absent, stools passed.
1st,September
C/o cough,cold.
INVESTIGATIONS

DIAGNOSIS
Autoimmune hemolytic anemia with thyroiditis(Hypothyroidism), pancytopenia with passive spleenomegaly,URTI.
MEDICATIONS